
Maintaining Oral Health: Frequently Asked Questions (FAQ)

- How do I tell if I have gum disease?
- What causes gum disease?
- How do I prevent gum disease?
- How can I tell I have brushed my teeth effectively?
- How is gum disease linked to cardiovascular disease?
- Are electrical toothbrushes better than manual toothbrushes?
- Isn't the fluoride in Singapore's water sufficient?
- Which mouthwash should I use?
- How often should I go for a preventive dental check-up?
- Why do x-rays need to be taken during dental check-ups?
How do I tell if I have gum disease?
Healthy gums are pink (rollover picture). In the initial stages of gum disease, it only affects the soft tissue surrounding the teeth (gingiva) hence the condition is called gingivitis. There is usually:

- Red gum margins that may be swollen or puffy looking.
- Bleeding gums — usually during tooth brushing as the bristles cross the swollen gums, and cause bleeding. On rinsing out after brushing, the blood-tinged water-toothpaste mixture looks pinkish-red.
- Bad breath.
When gum disease gets more severe, the infection spreads to affect the whole gingiva and tooth-supporting bone complex (periodontium), causing destruction of the bone supporting the tooth. This more severe condition is called periodontitis, and covers a spectrum from mild to severe periodontitis. At this stage, in addition to those described for gingivitis, there is also:

- Loose teeth as the supporting bone around the teeth gets destroyed, the tooth will get more mobile as less of it is anchored in the jaw bone.
- Drifting of teeth.
- Gum recession. (note: this may also occur without gum disease from traumatic tooth brushing habits.)
What causes gum disease?
Dental plaque is a soft, naturally occurring, invisible layer of bacteria that accumulates as a coating (biofilm) on teeth, is responsible for both gum disease and tooth decay (dental caries). Dental plaque is a complex colony of different kinds of bacteria, and different bacteria in plaque are responsible for gum disease and dental caries, the two most common dental problems. Some bacteria produce toxins that irritate the gums, causing gum disease, whilst a by-product of some bacteria, acid, softens and dissolve tooth structure. This tooth decay results in hole or cavity in the tooth.
When plaque is left undisturbed and is allowed to mature, it can utilise the calcium in saliva to form a hard, rough yellow to brown structure called calculus, or commonly referred to as tartar. Its rough surface makes it easier for more plaque to form on it, perpetuating the bacterial colony. Tartar is analogous to the adherent barnacles that colonise the hull of a boat. Unlike dental plaque, tartar cannot be removed by tooth brushing. Tartar needs to be removed professionally by a process called scaling.
The most common site for tartar to accumulate is behind the lower anterior teeth and the outer surfaces of the upper back teeth (molars).
How do I prevent gum disease?
Prevention can be achieved by:
- Tooth brushing effectively and regularly twice a day. Once in the morning and a second time before going to bed at night.
- Flossing to clean the areas between the teeth where the toothbrush bristles cannot, at least once a day before going to bed at night.
- Regular check-up with your dentist at a preventive recall period recommended commensurate with your susceptibility to both gum disease and tooth decay.
Some people, however, seem to be very susceptible to severe gum disease (periodontitis), despite apparently brushing their teeth effectively. There may be some genetic predisposition in such circumstances, and a link with increased risk of cardiovascular disease.
How can I tell I have brushed my teeth effectively?
Lift your lips to check after brushing. If there still is any debris between your teeth or along the gum line, you have missed these areas.
A more graphic method of evaluating the effectiveness of your brushing is to stain the almost invisible layer of plaque. If this is performed after brushing, it will show you the areas you have missed. Plaque can be stained using plaque disclosing tablets (available from pharmacies or dentists) so that it becomes obvious. Apply Vaseline onto your lips first so that they will not stain too. Chew the tablets as per manufacturer's instructions, then rinse out. Now look into the mirror.....

You can do the same thing using any red, green or blue liquid food dye that you may already in your kitchen. After brushing your teeth, take a cotton bud and soak one end into some food dye. Apply the dye onto your tooth surfaces. Rinse out. Inspect to see the areas you missed ....... brush again until the stained plaque is removed.
Tip: Do not try disclosing plaque before you go out, otherwise you'll get a lot of quizzical looks and have to explain why you have a coloured tongue (and lips if you forgot to put Vaseline!)
How is gum disease is linked to cardiovascular disease?
Recent evidence has demonstrated similar bacteria that cause severe gum disease, periodontitis, in the fatty deposits that accumulate in the blood vessels (arteriosclerosis). Should some of these deposits break off, they could lodge in one of the smaller arteries, blocking off blood supply to the affected part of the heart or brain, causing a heart attack or stroke respectively, collectively known as cardiovascular disease (CVD).
Originally, scientist thought this accumulation of fatty deposits that clog the blood vessels was related mainly to diet. Now it has been elucidated that it may be initiated by a similar exaggerated inflammatory response to the bacteria responsible for severe gum disease, periodontitis, that gets into and circulates in the blood stream (Desvarieux et al. 2005).
How does oral bacteria get into the bloodstream? Trauma to inflamed gums, e.g. from tooth brushing, eating, and professional dental cleaning all can cause oral bacteria to get into the bloodstream. In people with severe gum disease, the body's exaggerated immune response to these circulating periodontitis-causing bacteria may result in scarring of the blood vessel walls that initiates this build-up of fatty deposits. People with uncontrolled severe periodontitis are 4.5x more likely to suffer from CVA.
Periodontal treatment may prevent the onset or progression of CVD. Orthopantomogram dental x-rays may also show evidence of the arteriosclerotic build-up (Engebretson et al. 2005) in the carotid arteries, so that early treatment for CVD may be sought.
Are electrical toothbrushes better than manual toothbrushes?
Meticulous manual toothbrushing can be just as effective as using an electrical toothbrush. However, most of us are less than meticulous; or in a rush to work/school etc... in the mornings and can't wait to jump into bed in the evening. If you're in this category, then an electrical toothbrush could improve your effectiveness in the too short a time devoted to tooth brushing!(..... feeling guilty yet?)
There are different designs of electric toothbrushes. The two most common designs are:
- Rotation with oscillation
- Bristles move side to side
Studies show that only the rotation with oscillation type electric toothbrushes are superior to manual toothbrushing*. Examples of this are those from Philips and Braun. They do a great job that is also borne out in clinical studies. However, it can only clean areas where it is placed. So if you're missing areas of your teeth with your manual toothbrush and do the same with the electrical toothbrush, it won't be much help! Sorry..... no shortcuts there!
With all electrical toothbrushes, the vibration may initially turn you off (maybe it reminds you of dental treatment?). Persevere and you'll get use it........and indirectly to dental treatment!
Electric toothbrushes are especially beneficial for:
- Those with limited manual dexterity
- Children (or even adults!) who may not be motivated to brush. To them manual brushing is such a chore. The electric toothbrush - well that's a toy! Let's play with it!
*Robinson et al. 2005. Manual versus powered tooth brushing for oral health. Cochrane Database Syst Rev. 18;(2):CD002281.
Isn't the fluoride in Singapore's water sufficient?
Singapore's public water supply has been fluoridated since 1956. The current level of fluoride in the water is between 0.4-0.6 parts per million. This is for the systemic benefit of fluoride. The fluoride gets absorbed into the body and becomes incorporated into the developing teeth of children — so that when the teeth later emerge into the mouth, they will be more resistant to dental caries (cavities). Fluoride from toothpaste, on the other hand, has a much higher concentration of fluoride to provide a topical effect.
Which mouthwash should I use?
There are many different types of mouthwashes. Mouthwashes for general daily use are really not necessary, unless specifically recommended by your dentist. For example, fluoridated mouthwashes if you are caries prone, or chlorhexidene mouthwashes for gum disease.
If you are using a mouthwash to mask bad breathe or gum disease, you are only hiding the problem. It's best to see your dentist to determine the cause for your bad breath. Getting your cavities restored and improving the effectiveness of your brushing to prevent gum disease is will be more effective....and healthier for both your oral and financial health!
Furthermore, most commercial mouthwashes have a very high alcohol content, as it is both a solvent and preservative. When used long term, alcohol has the potential to cause undesirable changes to the oral tissues, although this has not been definitely proven. But what has been established is that alcoholism is one of the predisposing factors to oral cancer.
How often do should I go for a preventive dental check-up?
The frequency of dental check-ups depends on your dentist's risk assessment of your susceptibility to periodontal (gum) disease and dental caries (cavities), and the level of oral hygiene maintained. The guideline is:
| Caries Risk | Check-up Interval |
|---|---|
| Low | 12 months |
| Moderate | 6 months |
| High | 3 months |
Many dental problems are painless in their initial stages. Regular preventive check-ups allow any problems to be detected early and the appropriate treatment started. Waiting for obvious pain to develop usually means the problem is at an advanced stage, and consequently may require more complex treatment . This usually means higher costs. Ouch!
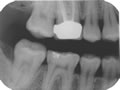
Why do x-rays need to be taken during dental check-ups?
During preventive check-ups, left and right bitewing radiographs (which record both the upper and lower teeth in one radiograph) may be taken to detect caries (cavities) between teeth and under existing restorations of the posterior teeth - areas where there is no/poor visual access for direct assessment. Available evidence suggests that the best cost-benefit for patients depend on their caries risk susceptibility. The current evidence-based guideline* is:
| Caries Risk | Check-up Interval |
|---|---|
| Low | 24 months |
| Moderate | 12 months |
| High | 6 months |
However, at various intervals, other radiographs may also be taken to monitor other conditions specific to you.
*Selection Criteria for Dental Radiography, Royal College of Surgeons (UK), 2000.
🔝